Food and Nutrition Services
 The concept of ‘food is medicine’ has a long history, as illustrated by the Haitian proverb, popularized by Paul Farmer, “Giving drugs without food is like washing your hands and drying them with dirt”.
The concept of ‘food is medicine’ has a long history, as illustrated by the Haitian proverb, popularized by Paul Farmer, “Giving drugs without food is like washing your hands and drying them with dirt”.
While adequate food and nutrition are basic to maintaining health for all persons, good nutrition is crucial for the management of HIV infection. Proper nutrition is needed to increase absorption of medication, reduce side effects, and maintain healthy body weight. As the survival rate of PLWH has increased, research has identified the virus as an independent risk factor for cardiovascular, liver and kidney disease, several types of cancer, osteoporosis and stroke. Several HIV medications can cause nausea and vomiting and some can affect lab results that test lipids, kidney and liver function. These compounding health effects, caused by the virus and its medications, reinforce the important role a nutrient-rich diet plays in a patient’s overall care plan. Food insecurity is a source of chronic stress that has consequences to immunological functioning, as well as for mental health and reduced adherence to medical treatments. In addition, providing food and nutrition services can serve to facilitate access and engagement with medical care especially among vulnerable populations.
Food and nutrition services (FNS) are increasingly recognized as key to accomplishing the triple aim of national healthcare reform: lower healthcare costs, improved health outcomes for PLWH. As to health outcomes, in a statistically significant way, PLWH who are food insecure report more missed appointments for primary care, are less likely to be receiving medical care that meets minimum clinical practice standards, have lower CD4 counts and are less likely to have undetectable viral loads than the food secure. Undetectable viral loads prevent transmission 96% of the time, thus, FNS is key to prevention.1 Other research has shown that food insecurity is associated with increased morbidity and mortality among HIV infected persons.
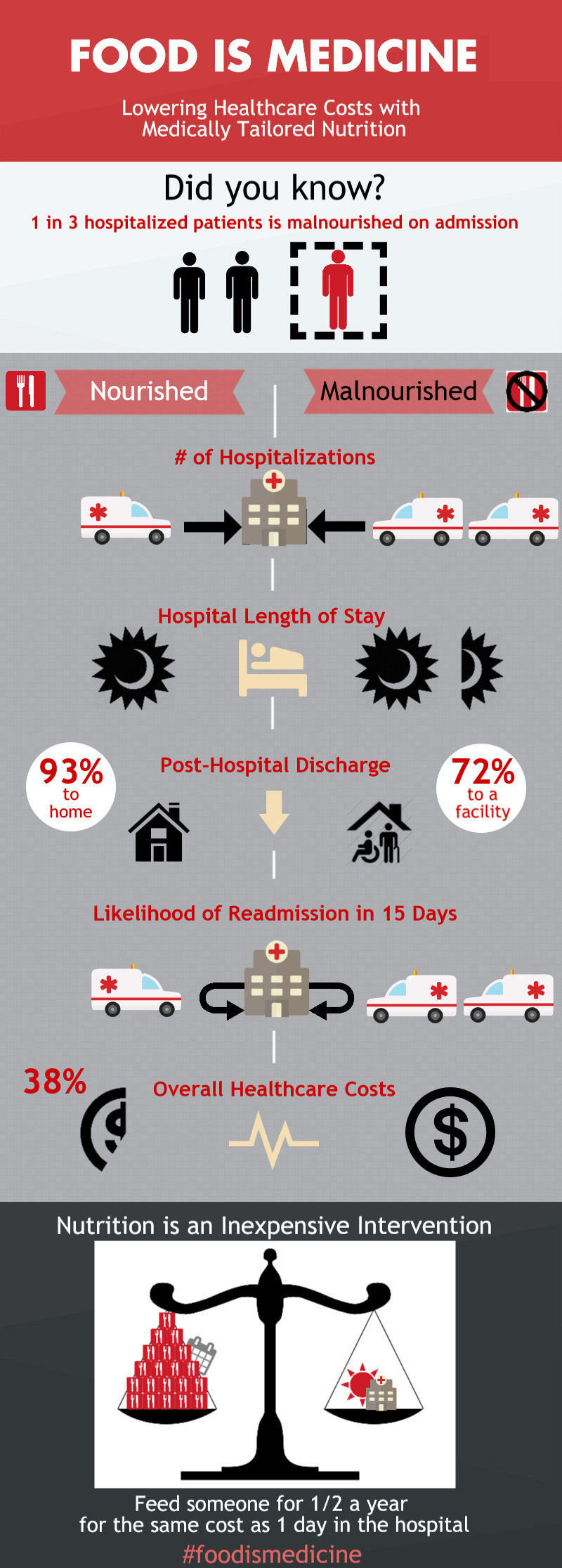
To put the cost savings of including FNS in medical care in perspective, a recent study comparing participants in a medically-tailored FNS program vs. a control group within a local managed care organization found that average monthly healthcare costs for PLWH fell 80% for first three months after receiving FNS. Furthermore, FNS is a very inexpensive intervention. For each day in a hospital saved, you can feed a person a medically-tailored diet for half a year.
Given the strong research and practice evidence in support of medically informed food and nutrition services, it is surprising that when the Patient Protection and Affordable Care Act (the ACA) was passed in 2010, it contained no comprehensive coverage of medically-tailored food for any severe disease population. From a policy perspective, the specific combination of a prescribed diet and the food that fulfills it is not integral to any program in either the Department of Agriculture (hunger-related issues) or the Department for Health and Human Services (healthcare issues), save the Ryan White Treatment Modernization Act (Ryan White). This lack of attention is despite explicit recommendations by the World Health Organization and UNAIDS that integrating food and nutritional supports are necessary for a comprehensive response to the global HIV epidemic, in high resource as well as under resourced settings.
If we are going to achieve a more coordinated national response to the HIV epidemic and our quest to reduce healthcare spending nationwide, FNS must be included in all healthcare reform efforts, including the Ryan White and the ACA. Ryan White remains crucial for the prevention and treatment of HIV/AIDS, even with some integration of food and nutrition services in the ACA through Medicaid. There remains a tremendous variation by state in coverage of food and nutrition outside of Ryan White. Even with some progress on coverage of medically-tailored home delivered meals within the ACA and state Medicaid Expansion, funding options for key services like pantry bags and congregate programs, which also support care and treatment, will be more difficult to secure.